PCOD headaches, hormonal fluctuations PCOD, frequent headaches PCOD, PCOD migraine causes, PCOD headache treatment, polycystic ovary disorder headaches, PCOD hormonal imbalance, PCOD headache remedies, insulin resistance headaches, PCOD lifestyle changes, PCOD headache triggers, chronic inflammation PCOD, menstrual migraines PCOD, PCOD headache prevention, PCOD diet for headaches
Frequent Headaches and Hormonal Fluctuations in Polycystic Ovary Disorder (PCOD)
Polycystic Ovary Disorder (PCOD), also known as Polycystic Ovary Syndrome (PCOS), is a prevalent endocrine condition affecting approximately 5–13% of women of reproductive age worldwide. Characterized by hormonal imbalances, irregular menstrual cycles, and ovarian cysts, PCOD significantly impacts physical and psychological health. Among its myriad symptoms, frequent headaches and migraines are increasingly recognized as debilitating issues for women with PCOD. These headaches are often linked to hormonal fluctuations, insulin resistance, and chronic inflammation, which are hallmarks of the disorder. This article explores the scientific underpinnings of frequent headaches in PCOD, their connection to hormonal imbalances, and evidence-based strategies for management, providing clear guidance for the general public.
Understanding PCOD: A Hormonal and Metabolic Disorder
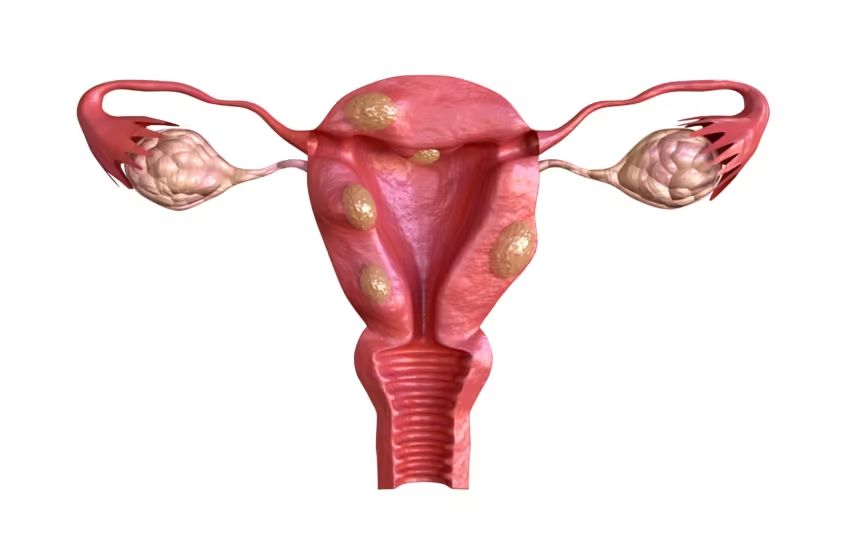
PCOD is a complex condition defined by a combination of clinical and biochemical features. According to the Rotterdam criteria, a diagnosis requires at least two of the following: hyperandrogenism (elevated male hormones like testosterone), ovulatory dysfunction (irregular or absent menstrual cycles), and polycystic ovarian morphology (multiple small cysts on the ovaries detected via ultrasound). These criteria highlight the hormonal and reproductive disruptions central to PCOD.
Hormonal imbalances in PCOD involve elevated levels of androgens, luteinizing hormone (LH), and insulin, alongside reduced levels of follicle-stimulating hormone (FSH) and sex hormone-binding globulin (SHBG). These disruptions lead to symptoms such as hirsutism (excess hair growth), acne, weight gain, and infertility. Additionally, up to 70% of women with PCOD exhibit insulin resistance, which exacerbates hyperandrogenism and contributes to metabolic complications like type 2 diabetes and cardiovascular disease.
Frequent headaches in PCOD are not merely coincidental but are intricately tied to these hormonal and metabolic disturbances. Women with PCOD often report headaches ranging from mild tension-type headaches to severe migraines, particularly around menstrual cycles or during periods of stress. Understanding the mechanisms behind these headaches is crucial for effective management.
The Link Between Headaches and Hormonal Fluctuations in PCOD
Headaches in PCOD are multifactorial, with hormonal fluctuations playing a pivotal role. The primary hormones implicated include estrogen, progesterone, testosterone, and insulin, each contributing to headache pathogenesis through distinct pathways.
1. Estrogen and Progesterone Imbalances
Estrogen and progesterone are critical regulators of the menstrual cycle and influence neurological function. In PCOD, irregular ovulation leads to erratic estrogen and progesterone levels, often with a relative estrogen dominance due to low progesterone. Estrogen fluctuations, particularly sharp declines before menstruation, are well-documented triggers for migraines. These drops affect serotonin levels and vascular tone in the brain, leading to headache onset.
Research indicates that women with PCOD experience migraines more frequently 2–3 days before or during the first few days of menstruation, correlating with estrogen withdrawal. Estrogen modulates pain pathways by influencing the trigeminovascular system, which is implicated in migraine pathophysiology. Progesterone, on the other hand, has a calming effect on the brain, and its deficiency in PCOD may exacerbate headache severity.
2. Hyperandrogenism
Elevated androgen levels, a hallmark of PCOD, contribute to headaches indirectly by promoting inflammation and altering pain perception. Androgens can enhance the release of pro-inflammatory cytokines, such as interleukin-6 (IL-6) and tumor necrosis factor-alpha (TNF-α), which sensitize pain pathways in the brain. This chronic inflammatory state may lower the threshold for headache triggers, making women with PCOD more susceptible to migraines and tension-type headaches.
3. Insulin Resistance and Glucose Dysregulation
Insulin resistance, prevalent in 50–70% of PCOD cases, is another key contributor to headaches. Elevated insulin levels disrupt glucose homeostasis, leading to blood sugar fluctuations that can trigger headaches. Hypoglycemia or hyperglycemia affects cerebral blood flow and neuronal activity, precipitating headache episodes. Moreover, insulin resistance amplifies inflammation and oxidative stress, further exacerbating headache frequency and intensity.
4. Chronic Inflammation
Chronic low-grade inflammation is a common feature of PCOD, driven by insulin resistance, obesity, and gut dysbiosis. Inflammatory markers like C-reactive protein (CRP) and cytokines are elevated in PCOD, contributing to systemic effects, including headache development. Inflammation can activate the trigeminal nerve, a key player in migraine pathology, and increase central sensitization, making headaches more frequent and severe.
5. Sleep Disturbances and Stress
Women with PCOD are at higher risk for sleep disorders, including obstructive sleep apnea and insomnia, which are linked to headache exacerbation. Poor sleep disrupts hormonal regulation and increases stress hormone levels, such as cortisol, which can trigger migraines. Psychological stress, often heightened in PCOD due to body image concerns and infertility, further amplifies headache risk by activating the hypothalamic-pituitary-adrenal (HPA) axis.
Scientific Mechanisms of Headache Pathophysiology in PCOD
To understand why headaches are prevalent in PCOD, it’s essential to delve into the neurobiological and vascular mechanisms involved.
Trigeminovascular System Activation
The trigeminovascular system, comprising the trigeminal nerve and its connections to cerebral blood vessels, is central to migraine pathogenesis. In PCOD, hormonal fluctuations and inflammation activate this system, leading to the release of neuropeptides like calcitonin gene-related peptide (CGRP). CGRP causes vasodilation and neurogenic inflammation, resulting in the throbbing pain characteristic of migraines.
Serotonin Dysregulation
Serotonin, a neurotransmitter, modulates pain and mood. Estrogen influences serotonin receptor expression and metabolism. In PCOD, erratic estrogen levels disrupt serotonin homeostasis, lowering the pain threshold and increasing migraine susceptibility. This is particularly evident during menstrual phases when estrogen levels plummet.
Cortical Spreading Depression
Cortical spreading depression (CSD) is a wave of neuronal depolarization implicated in migraine aura. Hormonal imbalances in PCOD may enhance CSD susceptibility, particularly in women with migraine with aura. Estrogen’s role in modulating neuronal excitability suggests that its fluctuations in PCOD contribute to this phenomenon.
Vascular Dysregulation
Hormonal imbalances and insulin resistance in PCOD affect vascular endothelial function, leading to impaired cerebral blood flow regulation. This dysregulation can trigger migraines by altering the balance between vasoconstriction and vasodilation in cranial blood vessels.
Clinical Presentation of Headaches in PCOD
Headaches in PCOD vary in type, frequency, and severity. The most common types include:
- Migraines: Characterized by unilateral, throbbing pain, often accompanied by nausea, photophobia, and phonophobia. Migraines in PCOD are frequently menstrual-related, occurring around the perimenstrual period.
- Tension-Type Headaches: Present as bilateral, pressing pain, often described as a “tight band” around the head. These are linked to stress and sleep disturbances in PCOD.
- Cluster Headaches: Less common but severe, these involve intense pain around one eye, often with autonomic symptoms like tearing or nasal congestion.
Women with PCOD may also experience chronic daily headaches, defined as headaches occurring on 15 or more days per month. The chronicity is often driven by a combination of hormonal triggers, inflammation, and lifestyle factors.
Diagnosis of Headaches in PCOD
Diagnosing headaches in PCOD requires a comprehensive approach, as they may stem from multiple causes. Key steps include:
- Medical History: A detailed history of headache characteristics (frequency, duration, triggers, and associated symptoms) and PCOD symptoms (menstrual irregularities, hirsutism, weight gain) is essential. Clinicians should inquire about menstrual cycle patterns, as headaches often correlate with hormonal shifts.
- Physical Examination: Neurological examination to rule out secondary causes of headaches, such as brain tumors or vascular abnormalities, is critical. Assessment of PCOD-related signs, like acne or acanthosis nigricans, supports the diagnosis.
- Laboratory Tests: Blood tests to measure hormone levels (testosterone, LH, FSH, estrogen, progesterone, insulin) and glucose metabolism (fasting glucose, HbA1c) help confirm PCOD and identify metabolic contributors to headaches.
- Imaging: Pelvic ultrasound to detect ovarian cysts is part of PCOD diagnosis. In cases of atypical headaches, brain imaging (MRI or CT) may be warranted to exclude other pathologies.
- Headache Diary: Patients are encouraged to maintain a headache diary, noting timing, triggers, and symptom patterns. This aids in identifying hormonal or lifestyle-related triggers.
Differential diagnosis is crucial, as conditions like thyroid dysfunction, hyperprolactinemia, or fibromyalgia may mimic PCOD-related headaches. Collaboration with an interprofessional team, including endocrinologists, neurologists, and gynecologists, ensures accurate diagnosis and management.
Management Strategies for Headaches in PCOD
Effective management of headaches in PCOD involves addressing both the headaches and underlying hormonal and metabolic imbalances. A multimodal approach, combining lifestyle modifications, pharmacological interventions, and complementary therapies, is recommended.
1. Lifestyle Modifications
Lifestyle changes are the cornerstone of PCOD and headache management, targeting insulin resistance, inflammation, and hormonal imbalances.
- Weight Management: Losing 5–10% of body weight can improve insulin sensitivity, reduce androgen levels, and alleviate headache frequency. A balanced diet rich in whole grains, lean proteins, and vegetables is recommended.
- Exercise: Low-impact exercises like yoga, Pilates, or walking enhance insulin sensitivity and reduce stress, mitigating headache triggers. High-intensity workouts should be avoided, as they may increase cortisol levels and exacerbate symptoms.
- Sleep Hygiene: Establishing a regular sleep schedule and addressing sleep disorders (e.g., sleep apnea) can reduce headache frequency. Avoiding caffeine and screen time before bed promotes better sleep quality.
- Stress Management: Techniques like mindfulness, meditation, or cognitive-behavioral therapy (CBT) help manage stress, a common headache trigger in PCOD.
2. Dietary Interventions
Diet plays a critical role in managing PCOD and associated headaches. Key dietary strategies include:
- Low-Glycemic Index (GI) Diet: Foods with a low GI, such as legumes, fruits, and whole grains, stabilize blood sugar levels, reducing insulin spikes and headache triggers.
- Anti-Inflammatory Diet: Incorporating omega-3 fatty acids (found in fish, flaxseeds) and antioxidants (berries, leafy greens) reduces inflammation, potentially decreasing headache severity.
- Gluten and Dairy Elimination: Some women with PCOD report symptom improvement, including reduced headaches, after eliminating gluten and dairy, which may trigger inflammation in sensitive individuals.
- Hydration: Adequate water intake prevents dehydration, a common headache trigger.
3. Pharmacological Treatments
Medications target both PCOD symptoms and headaches, tailored to the patient’s needs and reproductive goals.
- Hormonal Contraceptives: Combined oral contraceptives (COCs) containing estrogen and progestin regulate menstrual cycles, reduce androgen levels, and stabilize estrogen fluctuations, potentially decreasing menstrual-related migraines. However, COCs are contraindicated in women with migraine with aura due to stroke risk.
- Metformin: This insulin-sensitizing drug improves glucose metabolism and reduces androgen levels, addressing insulin resistance-related headaches. It is particularly effective in overweight women with PCOD.
- Anti-Migraine Medications: Acute migraine treatments include triptans (e.g., sumatriptan) and nonsteroidal anti-inflammatory drugs (NSAIDs) like ibuprofen. Preventive medications, such as beta-blockers (propranolol) or anticonvulsants (topiramate), may be prescribed for frequent migraines.
- Myoinositol: A natural supplement, myoinositol improves insulin sensitivity and has shown promise in reducing PCOD symptoms, including headaches, with fewer side effects than metformin.
4. Complementary and Alternative Therapies
Complementary therapies can enhance headache management in PCOD:
- Acupuncture: Studies suggest acupuncture may regulate hormones and reduce migraine frequency by modulating pain pathways.
- Magnesium Supplementation: Magnesium deficiency is linked to migraines. Supplementation (400–600 mg daily) may reduce headache frequency, particularly in women with menstrual migraines.
- Herbal Remedies: Herbs like feverfew and butterbur have shown efficacy in migraine prevention, though their use in PCOD requires further research.
5. Psychological Support
PCOD is associated with increased risks of anxiety and depression, which can exacerbate headaches. Psychological counseling, support groups, or CBT can address emotional stressors, improving overall quality of life and reducing headache burden.
Preventive Measures for Headaches in PCOD
Preventing headaches in PCOD involves proactive management of triggers and underlying conditions:
- Regular Monitoring: Routine check-ups with healthcare providers to monitor hormone levels, glucose metabolism, and headache patterns ensure timely interventions.
- Trigger Avoidance: Identifying and avoiding headache triggers, such as certain foods (e.g., caffeine, MSG), dehydration, or irregular sleep, is critical.
- Hormonal Stabilization: Consistent use of hormonal therapies or lifestyle changes to stabilize estrogen and progesterone levels can prevent menstrual-related migraines.
- Inflammation Control: Anti-inflammatory lifestyle choices, including diet and exercise, reduce systemic inflammation and headache risk.
Long-Term Health Implications
Untreated PCOD and frequent headaches can lead to significant health consequences. Chronic migraines may impair quality of life, increase absenteeism, and contribute to mental health challenges. Moreover, PCOD’s metabolic complications, such as type 2 diabetes and cardiovascular disease, underscore the need for early intervention. Addressing headaches as part of PCOD management not only alleviates immediate symptoms but also mitigates long-term health risks.
Conclusion
Frequent headaches in Polycystic Ovary Disorder are a complex symptom driven by hormonal fluctuations, insulin resistance, chronic inflammation, and lifestyle factors. Estrogen and progesterone imbalances, hyperandrogenism, and metabolic dysregulation create a perfect storm for migraines and tension-type headaches, particularly around menstrual cycles. Effective management requires a holistic approach, integrating lifestyle modifications, dietary changes, pharmacological treatments, and complementary therapies. By addressing the root causes of PCOD and its associated headaches, women can achieve symptom relief and improve their overall health. Early diagnosis, regular monitoring, and collaboration with healthcare providers are essential for optimizing outcomes. Empowering women with knowledge and practical strategies fosters resilience and enhances their quality of life.
FAQs
Q1: What causes headaches in women with PCOD?
A1: Headaches in PCOD are primarily caused by hormonal imbalances, particularly fluctuations in estrogen and progesterone, insulin resistance, chronic inflammation, and stress. These factors activate pain pathways and lower the headache threshold.
Q2: Are migraines more common in women with PCOD?
A2: Yes, migraines are more prevalent in women with PCOD due to estrogen withdrawal during menstrual cycles, chronic inflammation, and insulin resistance, which sensitize the brain’s pain pathways.
Q3: How can lifestyle changes reduce headaches in PCOD?
A3: Lifestyle changes like weight loss, low-impact exercise, a low-glycemic diet, and stress management improve insulin sensitivity, reduce inflammation, and stabilize hormones, decreasing headache frequency.
Q4: Can hormonal contraceptives help with PCOD-related headaches?
A4: Combined oral contraceptives can stabilize hormone levels and reduce menstrual-related migraines in PCOD, but they are not suitable for women with migraine with aura due to stroke risk.
Q5: What role does insulin resistance play in PCOD headaches?
A5: Insulin resistance causes blood sugar fluctuations and inflammation, which disrupt cerebral blood flow and trigger headaches. Managing insulin resistance with metformin or diet can help.
Q6: Are there natural remedies for PCOD-related headaches?
A6: Natural remedies like magnesium supplementation, acupuncture, and an anti-inflammatory diet may reduce headache frequency. Eliminating gluten and dairy may also help in some cases.
Q7: How does sleep affect headaches in PCOD?
A7: Poor sleep, common in PCOD due to sleep apnea or insomnia, disrupts hormonal balance and increases stress, triggering headaches. Good sleep hygiene can mitigate this risk.
Q8: Can stress management reduce PCOD headaches?
A8: Yes, stress management techniques like mindfulness and meditation lower cortisol levels and reduce headache triggers, improving overall PCOD symptom control.
Q9: Should women with PCOD see a neurologist for headaches?
A9: If headaches are frequent or severe, consulting a neurologist alongside an endocrinologist or gynecologist is advisable to rule out secondary causes and optimize treatment.
Q10: Can PCOD headaches lead to chronic conditions?
A10: Chronic headaches in PCOD can impair quality of life and increase risks of anxiety and depression. Addressing PCOD and headache triggers early prevents chronicity and complications.
Bibliography
- Azziz, R., Carmina, E., Dewailly, D., et al. (2009). The Androgen Excess and PCOS Society criteria for the polycystic ovary syndrome: The complete task force report. Fertility and Sterility, 91(2), 456–488. https://doi.org/10.1016/j.fertnstert.2008.06.035
- Stener-Victorin, E., & Deng, Q. (2021). Epigenetic inheritance of polycystic ovary syndrome — challenges and opportunities for treatment. Nature Reviews Endocrinology, 17, 521–533. https://doi.org/10.1038/s41574-021-00517-2
- Pourabolghasem, S., Najmi, S., & Arami, M. A. (2009). Polycystic ovary syndrome and migraine headache, is there any correlation? European Neurology, 61(1), 42–45. https://doi.org/10.1159/000165349
- Tural Balsak, B. Ö., Faki, S., Polat, Ş. B., et al. (2024). Insulin resistance in patients with polycystic ovary syndrome is a predictor of fibromyalgia. Reproductive Sciences, 31(1), 239–247. https://doi.org/10.1007/s43032-023-01347-0
- Silberstein, S. D., & Merriam, G. R. (1993). Sex hormones and headache. Journal of Pain and Symptom Management, 8(2), 98–114. https://doi.org/10.1016/0885-3924(93)90107-7
- Teede, H. J., Misso, M. L., Costello, M. F., et al. (2018). Recommendations from the international evidence-based guideline for the assessment and management of polycystic ovary syndrome. Human Reproduction, 33(9), 1602–1618. https://doi.org/10.1093/humrep/dey256
- Dennett, C. C., & Simon, J. (2015). The role of polycystic ovary syndrome in reproductive and metabolic health. Obstetrics and Gynecology Clinics of North America, 42(3), 561–576. https://doi.org/10.1016/j.ogc.2015.04.003
- Haqq, L., McFarlane, J., Dieberg, G., & Smart, N. (2014). Effect of lifestyle intervention on the reproductive endocrine profile in women with polycystic ovarian syndrome: A systematic review and meta-analysis. Endocrine Connections, 3(1), 36–46. https://doi.org/10.1530/EC-14-0010
- Allen, L. A., et al. (2022). Polycystic ovary syndrome: A review of mental health and quality of life impacts. Journal of Women’s Health, 31(4), 512–520. https://doi.org/10.1089/jwh.2021.0254
- World Health Organization. (2025). Polycystic ovary syndrome. Retrieved from https://www.who.int/news-room/fact-sheets/detail/polycystic-ovary-syndrome
Read More: Frequent Urination or Urge in Polycystic Ovary Syndrome (PCOS):